
Let's Talk About Sex, Baby!
What we know about sex and sexuality in transition

Foreword: This article talks about sex—including sex organs—and sexuality extensively, but in non-explicit ways. It’s not appropriate for minors to read.

Probably the most common questions I get about the trans experience, whether it’s from trans or questioning folks or their cis partners, are all about sex and sexuality. At the time of writing, two of the five most popular articles I’ve ever published are about this stuff, and there’s a constant call for more coverage. The questions people have really run the gamut from misconceptions about sexuality to fears about what will and won’t be possible in the bedroom; and they’re all super valid.
So… let’s talk about the big ones that come up, so to speak.
I don’t talk a lot about my own sex life or whatever I’ve got going on with my pelvis on Stained Glass Woman. It’s not that I’m ashamed or anything; I just like to have a little privacy for things like that. They feel special, sacred, tender to me, things I don’t really want to share with the world at large.
Unfortunately, that’s made for a bit of a doughnut hole in what I’ve covered so far, because Stained Glass Woman practices something called autoethnography, which is a way to do scholarly writing that uses the researcher’s—that’s me—own life to illustrate what these ideas look and feel like on a human level. It’s hard to wrap your head around the science behind minimization or gendering when we talk about it in the abstract; a human touch, it turns out, is really good at bridging that gap.
That’s not something I can really do for this article, and I thought you deserved to know why.
Before we get started, though, I need to slap a big ol’ disclaimer on what this is and is not going to be, and the limitations of our current research:
I’m going to cover both the transmasculine and transfeminine experience, but nonbinary realities are virtually unstudied in their entirety when it comes to sex and sexuality. This is unconscionable. It also means I can’t make evidence-based statements.
When it comes to nonbinary HRT regimens and their effects—we’re talking about things like microdosing hrt and combination testosterone and estrogen therapies—there’s just nothing out there at all.
A lot of what this article is going to talk about is generalities—some percent chance of this, some other percent chance of that, and so forth. No matter how high or low those percentages get, please keep the gambler’s fallacy in mind. Very unlikely things happen, and even extremely likely things sometimes fail to happen. That’s just how chance works.
A big part of transition, both for trans folks and our non-transitioning partners, is learning how to become comfortable with uncertainty—but that’s another article.
Human biology and sexuality are very, very weird, with a lot of expected unpredictability—and neither are as well-understood as you probably think they are. The half-life of knowledge applies really intensely here.
A really good illustration of this is the total change in what we thought we knew about trans brains in the last few years. Decades of what-we-thought-we-knew got thrown out.
Sex and sexuality for trans people are understudied, so the stuff I’ll be talking about won’t have the same strength of evidence that I usually have. So, please take all of this stuff with a healthy grain of salt.
Research on us has focused overwhelmingly on the risks that come with transition. Almost all of the remainder is about how beneficial it is for us. There just hasn’t been much funding to research things like lost hair coming back on estrogen, or what happens to our sex lives.
I’m using “transitioning” and “non-transitioning” to describe partners in a relationship in this article instead of “trans” and “cis,” because trans folks often find ourselves in romantic relationships with other trans folks. Sometimes that’s because we pair up and then realize our genders. Sometimes, one partner transitioning helps another realize that that’s what they need too. Sometimes, two trans people pair up, and only after a while does one decide to transition medically or surgically. As much of a surprise as it may be to folks, trans partners of transitioning people often struggle with these exact same worries.
These terms aren’t perfect, because sometimes both sides of a relationship can be transitioning at the same time. I couldn’t think of or find a better pair of terms to use.
I’ll be assuming dyadic—that means non-intersex—bodies and genitals when I talk about these things. This is not because I’m not aware of them, or that research has not been performed on those bodies. Far from it—the wide range of forms that an intersex body can come in means that the way they change in hormonal transition are often very diverse.
That diversity is very, very difficult to describe comprehensively, however; what a trans man with Swyer Syndrome can expect from testosterone might look very similar to what a dyadic person can expect, while a trans man with Complete Androgen Insensitivity Syndrome could expect virtually zero effect from testosterone. All of this is made worse because a huge portion of intersex people don’t know that they’re intersex.
I can’t do the diversity of their experience justice in an article around my normal length—I’d have to do a whole series of articles to do intersex trans realities justice—and regardless, the intersex community deserves much better than to have a dyadic (I’ve been karyotype tested, so I know for sure) trans girl act like she can speak for them. So, if you or your trans partner is intersex, I’d really encourage you to either speak to your doctors about it or, better yet, reach out to other intersex trans folks, to get a much more personal and true-to-you picture of what HRT’s effects might look like for you.
Sexuality in transition
I want to start with sexuality, because it’s often a big worry for trans and gender questioning folks who are thinking about transition, and it’s pretty much always a worry for their non-transitioning partners—will the transitioning partner stop being attracted to the non-transitioning partner? Will their sexuality change in transition?
It’s surprisingly hard to say whether or not sexuality changes in transition and, if it does, why. Some research has found that between 32% and 60% of all trans folks have a change in their sexualities in transition—not because of HRT, but because of transition itself. Other research, with a much larger study sample, found that “sexual orientation did not change during hormonal transition and was not associated with sex steroids or surgery.” What’s going on here?
Well, I’m part of that 32% whose sexuality “changed” in transition, and my story is surprisingly typical. When I went into transition, I was exclusively attracted to women. Now? Still exclusively attracted to women.
What gives, right?
I’m lesbian and demisexual, and it wasn’t until after I’d gotten well into my transition that I was able to look at my sexuality and realize I’d been on the asexual spectrum all along, but hadn’t been able to see it because of how bad my gender dysphoria was. And, once I’d already come out as being trans? Owning my demisexuality just… wasn’t a very big deal, by comparison. A lot of trans folks end up coming to their asexuality and bisexuality, pansexuality, or omnisexuality in the same way.
Here’s the good news for you: a partner in transition will almost certainly keep being attracted to their non-transitioning partner. I want to look at data from one part of Table 2 in that article a little more closely, on who trans folks are attracted to:
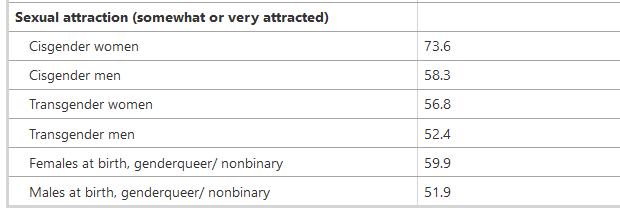
It’s pretty obvious here that trans people tend to have very inclusive attraction patterns. The same study found that 82.4% of all trans folks weren’t straight.
So, yeah. You’re probably going to be just fine.
Now, there’s one other bit that I should probably talk about here: consensual non-monogamy—most notably, polyamory. Around 5% of all adults in America, which is the best-studied country, are currently in a consensually non-monogamous relationship, but that rate is much higher among trans folks: around 32%. That may sound like a huge difference, but 27.5% of all Americans either have done CNM before or are interested in it. I’m mentioning it here because many polyamorous people feel that it’s a sexual orientation, fundamentally no different than their core sexuality. Others disagree. It’s complicated, and contested.
Anyway, this is a case that’s a lot like trans people being much more likely to not be straight than cis people: once you’re out as trans? Practicing CNM just isn’t as big a taboo as being trans is, so it just doesn’t seem as extra-scary to trans folks as it does to cis folks. Just a thing to be aware of.
Desire on HRT
One thing that a lot of people don’t expect is how sexual desire itself can change in transition—and how it doesn’t. Transmasculine people who start HRT are typically warned about major increases to sexual desire, while transfeminine people are usually warned that theirs will crater. It makes sense, in a napkin-math sort of way, because testosterone levels are directly linked to libido.
The reality is vastly more complicated, because libido is one of the more complicated multifactoral systems in the human body.
Our best research to date on trans desire and sexual satisfaction found that there’s usually a decrease in sexual desire for trans people when they start HRT… during the first three months of hormonal transition.
But.
But three years after they started HRT, trans folks had identical desire and sexual satisfaction to what they had before transition. What’s going on here?
Well, hormonal transition is a stressful time, both physically—the transitioning person’s whole body is changing, after all—and socially. And stress? Stress kills libido. Generally speaking, the best thing to be done in what feels like a dead bedroom is to tend to the other things going on in life for both partners, because transition is stressful on everyone in a relationship. When things settle down, libidos will come back. It just takes time.
Now, what’s also common is that the ways a trans person will want to have sex will change a lot too. Some of that is how HRT affects our erogenous zones—more on that in a minute—and some of it is going to be a trans person letting go of the ways they were told they “should” have sex and getting more in tune with how they want to have sex. There’s a great book I’ll talk more about later on called Come Together that can be a wonderful help in exploring what this might look like in your relationship.
Changes downstairs
I’m going to be really up-front here: HRT will almost certainly affect a trans person’s genitals. Now, that’s not to say that these precise things will happen, and in the exact same way, to everyone on HRT—biology is messy, and exceptions to literally every condition or status possible in a human body will exist. Big differences from person to person aren’t just expected, they’re normal.
But these changes are just part of the overall effects of hormone replacement therapy.
Now, that doesn’t mean you won’t have options.
Transmasculine folks
The main, and most obvious change, that transmasculine people can expect is that with enough time on testosterone, their clitoris will grow into something many trans men refer to as a T-dick. Less obviously, however, the lining of the vaginal canal will slowly atrophy, which often makes penetrative sex more painful when the transmasculine person is the receptive partner. In addition, a transmasculine person’s body will usually produce less lubrication when they’re aroused, which can make this problem worse. The types of sensations that they find pleasurable will usually become a lot more like the types of sensations that cis men find pleasurable. Finally, transmasculine people on testosterone usually say that their experience of orgasm changes, becoming the same as what cis men experience. This often includes losing the ability to have multiple orgasms in a single sex act, but not always.
Sorry for being a little vague here, but there isn’t much more I can do without getting explicit to a degree I’m just not comfortable with. Go check out Come Together if you want the details.
So, if a transmasculine person wants to mitigate this stuff—and especially the vaginal atrophy—what can they do? Well, weirdly enough, the simplest thing is to talk to their doctor and get a prescription for the exact same low-dose (I want to emphasize that, because it’s made to stay local to the important bits and won’t mess up your hormonal transition) topical estrogen cream that docs prescribe to their elderly cis women patients facing the same problems. It goes right on the genitals and stays in that area, rather than getting around the whole body and interfering with what testosterone is doing to the rest of their body.
If that’s not your speed, there are some moisturizers that you can usually find in the sexual health section of your local drugstore or pharmacy that are formulated to be gentle enough to be used on your genitals. It’s important to not use them too frequently, though—only once every 1-3 days—because the microbiome down there is a little delicate at cisfeminine estrogen levels, and becomes even moreso when your estrogen gets dropped from HRT.
Beyond that? Using a generous amount of water-based lube during sex is a really good move, or having the transmasculine person not be a receptive partner during sex.
Transfeminine folks
Transfeminine people are going to see a wider variety of obvious genital changes than transmasculine people because of the way our typical factory default genitals are put together.
The first and most noticeable change most transfeminine people see is a loss of nocturnal erections, which is usually followed by an inability to have an erection, or at least an erection suitable for penetrative sex, at all. If that’s not something that you want, I’ve got a whole article on how to work to prevent it, but a lot of transfeminine people who feel bottom dysphoria eagerly welcome these changes, so it’s really important to have an open and honest talk with your partner about what they want.
This is especially important because, if a transfeminine person doesn’t regularly have erections, her penis will slowly atrophy. Not in a dangerous way, to be clear! But it will shrink and become permanently unable to become significantly erect, and will usually feel significant pain when their body tries to have an erection. Again, many transfeminine people with bottom dysphoria welcome this change; many do not.
Open and honest conversations, remember?
Now, we know that this change happens, but we’re not 100% sure of its cause. Probably what’s going on is that the elastic parts of her penis are experiencing fibrosis, and losing the ability to be elastic in the way a penis needs to be to have an erection. Most of the research we have on this process was done on cis men who are recovering from testicular cancer, where their ability to make their own testosterone had to be killed.
A lot of non-transitioning partners get pretty worried about these changes, and they’re the source of the transphobic lie that trans people can’t have orgasms. This is false. In reality, not only can transfeminine people orgasm, their patterns become more or less identical to those of cisgender women, often gaining the ability to have multiple orgasms. The key, for non-transitioning partners looking to have great sex, is to treat a transfeminine person’s penis as though it were just a big clitoris.
Again, I can’t get into much more detail without getting really explicit. Go check out Come Together if you want the details.
One last bit: a transfeminine person’s testicles will slowly shrink while she’s on estrogen. This is almost universal, and I’ve never seen a report that says there’s any pain or trouble with it, or that this change has had much of any effect in the bedroom.
Let’s talk fertility
A lot of trans folks want to be parents someday, just… not quite yet. And that’s great! But when a trans person is about to start HRT, it might be a really good idea to give some careful thought about what they might want, because HRT will mess with their ability to become a parent in… the traditional way, shall we say. Trans folks who go in to start HRT will usually be told that the HRT will make them sterile.
This is not true. I cannot emphasize this enough. About 24% of all trans people will remain fertile enough for it to be possible for a child to be conceived.
So, if you want to have a kid someday or think there’s a reasonable chance, assume HRT will indeed make you sterile, and take some precautions. And if you don’t want a kid? Use birth control.
Transmasculine folks
One of the main things that happens for transmasculine people on HRT is that dropping estrogen and ramping up testosterone will almost always stop their periods for as long as they stay on HRT. In turn, this usually but not always stops his ovaries from releasing eggs. Once in a great while, a guy who hasn’t had a period in a long time will suddenly find himself pregnant—in which case, he’ll need to pause his testosterone until he gives birth if he wants to keep the baby.
The really good news for transmasculine people who want to carry a child is that they can usually regain their full fertility in pretty short order by pausing their testosterone; as soon as they have a full, normal period, they’re good to go. The term that seems to have caught on for these guys is Seahorse Dads, after the documentary, which I think is wonderful.
Transfeminine folks
Transfeminine folks have been told for a long time that if they’re on HRT for a long time, that they’ll become permanently sterile. This is false—we’ve seen full fertility restoration, unaided by anything other than simply pausing HRT, in a trans woman who’d been on HRT for eighteen years. As with transmasculine people, pausing HRT for as little as three months is often enough for a transfeminine person to regain her full fertility. Now, there are cases where things come back much more slowly (as much as a year), and she may need some medical assistance to extract sperm that can be used to conceive a child, but it’s clear at this point that the assumption of long-term permanent sterility is simply false.
All that being said, cryopreserving sperm is a tried and true technology, so if a transfeminine person wants to be a mother to her biological kids someday, it’s a really, really good idea for her to freeze some material before she goes on HRT so that she won’t have to stop. A trans woman I’m friends with from grad school became a mother a few years ago this way, and watching her dote on her child is one of the more heartwarming things I’ve been lucky enough to get to watch.
The last thing I want to take a few moments to talk about here is much harder. Many transfeminine people experience uterine dysphoria, meaning that they feel gender dysphoria because they cannot carry and birth a child. Transfeminine people who feel this kind of dysphoria often hope that they can address it with a uterus transplant, now that uterine transplants are possible and accessible for cisgender women who need them to carry. This dysphoria is common enough that Lily Elbe was, in 1931, the first woman, trans or cis, to ever receive a uterine transplant.
And she died because of it.
Unfortunately, this hope is often based on a poor understanding of how uterine transplants are performed today, their limitations, the fact that the transplanted uterus is always removed after the child it was implanted for is born, and that doctors won’t even attempt a transplant to a woman who’s older than 40. Just as importantly, there is not a tested and reasonably safe way to perform these transplants on transgender women, as abdominal muscles and blood supply develops a little differently when someone grows up on testosterone than they do when someone grows up on estrogen.
These aren’t showstoppers, to be clear. These are solvable problems. But they’re not problems we have solved, they won’t be solved for many years, and until we’re well into the era of organs grown from a person’s own stem cells (and, therefore, which their body won’t reject), nobody, trans or cis, will have a transplanted uterus that they keep for the remainder of their life.
Personally? I wouldn’t bet on the first successful uterine transplant into a trans woman happening sooner than ten years from now.
I mention all this not to hurt anyone, but because the people who feel this type of dysphoria deserve to know what the state of our medicine really is and is not. Most people get into healthcare because they want to help people, but some do it because there’s a lot of money there. To be really frank, there aren’t many places in all of healthcare where people are more willing to spend money than infertile folks desperate to birth a child, which means that’s one of the places where the shady folks who do slip through the cracks and into medical practice tend to self-sort themselves into.
This is an area where folks need to be careful of anyone making big promises.
Go to your local library!
Most importantly, I want to suggest that you keep reading, learning, and exploring, whether you’re trans or a trans person’s partner—and there’s two really wonderful books that I think can help anybody, of pretty much any sexuality, find joy and fulfillment in the bedroom during transition, and one which will probably be a little more specialized.
The first one is Trans Sex, and it’s a wonderful book that reframes what really healthy and joyful trans sex and sexuality can look like. Really, the big downside of it is that it’s written not for trans folks and their partners directly, but for therapists, and so some of the language it uses can be a little thick to get through, and it assumes some knowledge that some readers might not have. If you’ve been through an intro to psychology class or took a human sexuality course in college, you should be all right with Trans Sex, but if not? Well…
Come Together is the most recent work of Emily Nagoski, whose work I think very highly of. It’s an absolutely wonderfully-inclusive book about pleasure-centered sexual connection for people of every type of body, trans or cis, and it’s written in wonderfully personal, accessible, welcoming language. The part I love best about it—and, I think, the part that’s most helpful for partnerships in transition—is that it encourages people to set aside any ideas they might have about what sex should look like, to explore what it can look like.
Finally, Polysecure is a book which has been spoken of in glowing terms by every polyamorous person I’ve met who’s read it. The core idea of the book is to encourage each partner in a romantic relationship to look deeply into how they form deep, lasting, secure romantic connections with other people in order to make those romantic connections more robust and longer-lasting. If polyamory peeks its head into your relationship, Polysecure is generally considered to be the gold standard for how to do things well. It’s based in a psychological idea called Attachment Theory that’s really well-regarded, and many polyamorous friends of mine even recommend it to monogamous couples looking to deepen their emotional and romantic connections—just, ignoring the bits about multiple partners.
I don't think you'll find it in your local library but F*cking Trans Women by Mira Bellweather was (at least for me) an enlightening resource when I was exploring myself after two years of estrogen. It is albeit a lot less clinical and more gritty than many of the resources you provide in your articles. Last time I checked, a quick Google search and you can find a PDF of her work.
Thanks, great as usual. Head's up, I'm going to talk about more body stuff, maybe someone will find it gross... When you were talking about testicle shrinkage "...I’ve never seen a report that says there’s any pain or trouble with it...". I'd like to mention something I've experienced and I know a limited number of other trans-femme people have also experienced this which is blood in the ejaculate (not that there's much). This amounts to a few drops of clear fluid with a dark brown tint (old blood) and occasionally a hint of pink from newer blood. It can be really disturbing when it's not expected, there's no pain with it. For me this started about 9 months into HRT. I was suitably concerned and talked to my Dr. who ordered an ultrasound of my prostate, bladder and kidneys to rule out any obvious tumours etc. Those came back fine. A urine test came back fine with no detectable blood, so not even microscopic amounts. We both did some research and came up with anecdotal evidence that this is not unheard of in transgender women. I don't know if it's related to the testicles or the prostate atrophying or something else but so far that's what we're chalking it up to. I'm currently at 11 months on my HRT journey and it comes and goes (I'm 55 if anyone is curious). Anyway, just wanted to add this for other peoples information.
I'd found an 8 year old post on Reddit where a couple of others chimed in with similar complaints but obviously not super common. My Dr. didn't specify exactly what her source was but I got the sense it was from talking to other doctors.
I hope this wasn't too much!
Leah