


Who We Are
What we're learning about being trans from the 2022 US Transgender Survey

Author’s note: I’ve had to be a lot more quick writing this article than I normally am, because of responsibilities elsewhere. Do please let me know if you notice something I’ve missed, or misstated.

If you’ve read any Stained Glass Woman at all, one of the things you’ve probably seen come up again and again and again is just how spotty so much of our research on being trans is. In some spots, like understanding the risks of surgery or hormones, our research is incredible, with detailed findings quite a bit superior to a lot of other things that medical researchers study all the time. In others, like timelines and effects of HRT? We’re really, really out of date.
And in a lot of ways, all of that makes sense. Trans people, according to our best counts right now, are somewhere around or a little higher than 1.6% of the world’s population. That’s a pretty small group of people. Historically, our doctors and psychologists have been pretty shitty to us, so big parts of the trans community are seriously distrustful of anyone in a white lab coat—and, worse, for a long time we had to lie to them in order to make our way through the bullshit gatekeeping system that they set up to try and keep us from transitioning. Add on top of that the simple fact that, even when you can get a trans person to agree to work with you as a doctor or a psychologist, following that trans person through, for instance, the entirety of transition is a 7-10-year project, and you run facefirst into a huge research problem:
Trans people are both uncommon and, mostly, we’re uncommonly expensive to study.
It makes a lot of sense why we’ve got these huge donut holes in our research. Researchers have hunted up the cheap and feasible things to study, because that’s what we tend to do—easy stuff first, then the hard stuff, once we can prove to grant boards that the hard stuff is worth funding. And unfortunately, given who’s ultimately banning whole areas of research these days and the merry ratfuckery they’re pulling with grant funding as a result, that’s not going to change for a while.
The 2022 United States Transgender Survey is really important in all of this for a couple of reasons:
It’s by far the largest study in history of transgender people, with 92,329 respondents. That’s almost triple the size of the next-largest survey ever conducted on trans people which was—you guessed it—the 2015 USTS.
It was run in connection with the National Center for Transgender Equality (which has since merged with the Transgender Legal Defense Fund, and is now known as Advocates for Trans Equality), an organization run by trans people and which is widely trusted by us.
It doesn’t rely on US federal grant funding.
So, when the most important parts of the 2022 United States Transgender Survey were released last week, you better believe that it’s one of the most exciting days in years, as a trans data nerd!
While some other folks have already taken some interesting top-line data from the report—and seriously, those articles are really worth reading—I want to dive a little deeper on the data, so we can understand what makes it tick and how things have changed between the 2015 and 2022 US Trans Surveys.
Yawn. Methods.
Yeah, I know, methods are boring. Thing is, they also tell us a HUGE amount about what the USTS is actually saying and, more importantly, what it’s not saying. We’re gonna move quickly, so you understand the basic limitations of the USTS when we dig in on the data in a few minutes.
Sampling
The USTS uses a refined version of snowball sampling to recruit people to take it. Basically, it’s the word-of-mouth equivalent of sociological research—”tell a friend” and all that. Snowball sampling is really, really good at getting big sample sizes, which is really important in a study like the USTS. There’s a big downside, though: it’s a nonprobablistic method, which is a fancy-pants way of saying that while it collects a really big sample, that sample both is not representative of the whole group, and which inherently cannot be used to talk about representativeness.
Yeah, that’s a buncha stats talk. Sorry. Methods. Not much else we can do here.
So, let’s illustrate it instead: when you do a snowball sample like this, friends get referred in, which is good. But people self-sort into groups of similar people and separate from dissimilar ones, which is why, for instance, trans guys and trans gals don’t run into each other, socially, as often as we run into other trans members of our own genders.
But that means that people who aren’t connected to those spark-points, at the start of the snowball? They tend to either show up less than they should, or get missed completely.
Region
There’s no two ways about this part: The USTS is about trans people living in the United States. Our demographics are going to be different than even some very similar countries, like Canada or France. Now, for something like transness, where the fact that we’re trans is comes from our genetics, this is less of a big deal. It becomes a bigger deal because in places like Russia, where modern understandings of transness are suppressed, people are a lot less likely to be able to figure out that what they’re feeling is Being Trans.
Social Media
Because it’s an online snowball study, the USTS relied a lot on social media websites—Instagram, Facebook, Tiktok, Twitter, and Tumblr, mostly. Not everyone uses those, or is active on them, and those slices get impacted really heavily by other stuff, like gender and age, that don’t have a whole lot to do with being trans.
The Bottom Line
So, what does this all mean about understanding what the USTS says? In a nutshell: we have to be careful about generalizing it too much. Because of how they ran it, they’re gonna get a disproportionately large number of chronically online trans dweebs like me, and a disproportionately small number of people who aren’t actively connected to online trans community.
That might just be because they’re nature nuts. It might also be because, for instance, they’re nonbinary, and don’t experience dysphoria which might make them more likely to reach out to online trans community for help in addressing it. The first? No biggie. The second? Really big deal, if what we want is representative data. This graph, from the Early Insights, is a really good example of that exact thing:
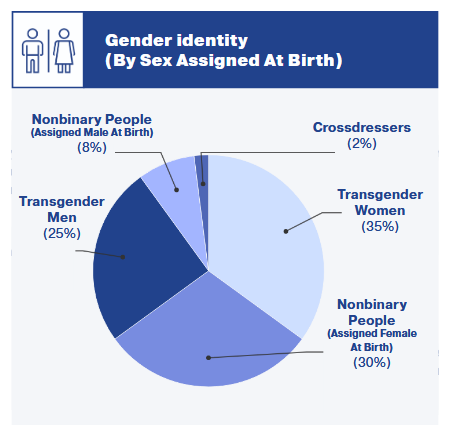
Look at how few nonbinary transfeminine people got sampled, compared to nonbinary transmasculine people! Other research we have has said pretty consistently that the nonbinary/binary breakdown is pretty even, or a 60/40 split favoring enbies, with a pretty even number of transmasculine and transfeminine enbies. It’s a special pleading to think that the USTS got it right and they got it wrong.
The sheer size of the USTS helps here, some—just, remember, there are going to be folks who aren’t well-represented by it. Keep that in mind when you’re making claims.
Shaddap, nerd. Get to the interesting stuff!
Okay, okay!
Joking aside, there’s a lot of strong confirmation of things we already knew about being trans. Let’s hit them in rapidfire!
Healthcare providers tend to treat us crappier than they treat cis people, and it shows up in our overall health. We’re much more likely to evaluate our health as “fair” or “poor” than the general population, and 47% of us were disrespected in the last year for being trans.
27% of the people who told their doctor that they were trans felt disrespected because of it within the last year. This is an improvement from 2015, but not a huge one.
Unsurprisingly, trans men and transmasculine nonbinary people are the people who get disrespected most often. A whopping 32% of trans men hadn’t seen a doctor in the last year specifically because they expected to be disrespected or mistreated.
Almost a fifth of us—18%—had to teach our doctors basic stuff about being trans in order to get basic care. That’s horrifyingly high.
Even among those of us who see a specialty doctor for trans-related heathcare, 23% of us had specialty providers who didn’t know the things we needed them to know.
We tend to get beaten up by the healthcare system: 21% of respondents hadn’t seen a doctor in the last year. That puts us at much higher risk for a whole lot of things.
Shocking absolutely nobody, cost is the biggest reason here, followed by doctors being crappy to us.
About 60% of all respondents had done some level of medical transition, but 88% wanted HRT, whether they’d had it or not.
This one might be one to be cautious about because of sampling. For example, if the USTS undersampled transfeminine enbies—and it looks like it did—then nonbinary people are the group of trans folks least likely to want HRT or surgery of some form. That’d make a pretty big dent in the numbers here.
Basically nobody who starts HRT or gets a gender-affirming surgery regrets it. One percentage point or less for all regrets in either case.
Fertility counseling before starting HRT seems to be excellent—95% of everyone who saw a doctor for HRT had a chance to talk about fertility needs.
It’s hard being trans these days. We’re about eleven times more likely to meet the criteria for depression than cis people—44% versus 4%.
Given that 78% of trans people wanted the help of a therapist and only 48% were able to get it, this shouldn’t be surprising. Dysphoria and minority stress are a brutal combination.
Worse yet, 12% of those who’d managed to get access to a therapist were faced with conversion therapy in response. A staggering 50% of all religious therapists attempted conversion therapy.
We also seem to have trouble staying in therapy, probably because of costs. Only 67% of those who managed to get in and see a therapist in the last year were still seeing one.
Suicidality is a problem in the community, and it’s highly linked to how often we get attacked, harassed, and discriminated against. For instance, 63% of those who were the victim of a transphobic assault in the last year considered suicide.
In short, the USTS confirms the findings of a whole bunch of other studies on trans mental health: our struggles with mental health and suicidality come directly from other people treating us like shit.
While we struggle with happiness in many areas, there’s a pretty direct relationship between how far someone’s gotten in their transition—social, not just medical!—and how happy they are overall.
For example, over 36% of respondents who were in social or medical transition said they were thirving, the highest satisfaction metric the USTS offered. This was twice the rate of those not in transition.
So, how have things changed since 2015?
There’s also been a lot of huge changes in the data since 2015, and a lot of them are either really interesting or just plain great news. Let’s get to it!
Detransition data!
One area that’s critically understudied in trans research is the rate of detransition. It’s hard to find detransitioners, and they’re a small portion of a small population. Thanks to the USTS, though, we’ve got some better data than we’ve had almost anywhere.
9% of respondents, so almost 1 in 10, detransitioned at some point. When you dive into those numbers, though, virtually all of them had detransitioned due to safety, social support, or for employment. Only 0.36% of those who’d medically transitioned at any point detransitioned at all, for any reason.
What this all means is that the main barrier to transition is at the start of things—coming out to our families, workplaces, and so forth. If we can navigate those obstacles, we generally seem to be able to manage our transitions.
And that means that it’s important for the community, and for providers, to make an extra special effort to be gentle and helpful to those early on.
Messy datapoints when it comes to age
This one’s a caution: the 2022 USTS has a lot of data in it sorted out by age, which the 2015 USTS didn't do very much. Most of it says that the older you are, the happier, healthier, safer—pretty much every good metric you could ask about—you are. Problem is, this is generally true of every study that breaks things down by age, because young people are poorer than older people. If you’re poorer, you can't see a doctor as often, you’re gonna struggle with paying for medications, you’re gonna be stuck working crappier jobs and in worse living situations, and so on.
This is what we call an independent variable, folks. There’s stuff not related to the thing you’re measuring (being trans) influencing the results in ways we can’t control for. Don’t put too much weight on this.
Family support matters
I could talk this up a lot, but honestly, the USTS’ graph, despite an inexplicable typo on “Neutral,” tells the story more clearly than I could. The more supportive your family is, the better your health is going to be.
.\" 69% of people with supportive families were in good or better health, compared to only 56% of those with unsupporitve families.")
There’s gonna be a lot of reasons for this, but let’s cover the most basic and important ones. Trying to get well when you’re not at your best is hardest when you’re on your own, and that tends to make health problems snowball. But more than that, just basic stress, which is alleviated by transition and made worse by family being shitty, is a chemical chain reaction throughout the body that damages every part of yourself.
Insurance (ugh)
Insurance coverage denial rates plummeted from 2015! This is sharpest in the surgical data, but across the board, denial rates dropped by more than half—HRT denials dropped from 25% to 11%, and surgical denials dropped from 55% to 20%!

There are still a lot of donut-hole coverage problems with insurance, though—it seems that partial coverage of transition care remained more or less the same, changing little from 42 to 45%. This could refer to copays, but might also represent insurance companies knowing they can’t get away with most denials anymore as a result of WPATH SoC8, which most of them are bound to by contract, and shifting their coverage strategy from outright denials to minimal coverage.
What surgeries are people having?
Since WPATH Standards of Care Version 8 forced open the doors to coverage for many trans people—even though it had only been in effect for a couple of years when the 2022 USTS was opened for responses—the numbers of who’s getting surgery, and what, have changed in some very interesting ways.
Let’s start at the top: in 2015, 25% of respondents had gotten some form of gender-affirming surgery, and the USTS didn’t make clear what percentage wanted some form of surgery—they just broke it down by type, but since one person can want multiple forms of surgery, it’s not possible to get to a topline number from there. In 2022, 31% had managed to have at least one gender-affirming surgery, while a whopping 84% wanted one.
This shouldn’t come as a surprise. 57% of transmasculine people wanted top surgery, and 55% of transfeminine people wanted laser hair removal, which the USTS lumps in for these purposes. Those two procedures alone more or less guarantee a supermajority of trans people who want surgical interventions, especially when you include the 20% of transmasculine people who’ve already had top surgery and the 34% of transfeminine people who’ve already had facial hair removal.
Let’s break things down by categories, since “top surgery” means more or less opposite things for transmasculine and transfeminine people. Here’s what transmasculine people reported on surgeries in 2015:

And in 2022:

In many ways, the data here has remained pretty much the same. About one in five transmasculine people have been able to get top surgery, and only about 8% have been able to get a hysterectomy. The main difference between the two is that the newer survey includes a lot more specific information for other procedures than the 2015 data captured, which will be very helpful for the next USTS.
And now, here’s what transfeminine people reported on surgeries in 2015

And in 2022:

Again, the numbers are really steady, which came as a bit of a surprise to me.
Here’s the thing though: if a 25% larger percentage of the trans population have gotten procedures of some kind, why are the percentages of those having gotten them lower in many cases? And especially when so many more doctors are performing gender-affirming surgeries than there were in 2015!
It’s possible there was a typo somewhere, of course—that happens from time to time. Secondly, it's very likely that in the 2015 USTS, it was more common for a single given trans person to have had several different procedures, like I have, and in the 2022 USTS it was more common for a single given trans person to have had only one. This is probably because there’s been a huge increase in the US trans population since 2015, spiking in 2020-2021, which has more or less tripled our headcount.
That’s gonna create some bottlenecks, no matter how many surgeons you have out there. So, yeah, a lot of people have gotten surgeries—a larger percentage of the total population than in 2015. And also, when they took this survey, there were a whole lot of early-transition folks who may not have been physically, financially, or emotionally ready yet, or hadn't had the chance to have everything they wanted.
This stuff is complicated.
We are who we thought we were
I guess, in the end, the most important finding of the 2025 USTS’ health and wellness research is simply this: it turns out that trans people are exactly who we say we are, our problems are for the exact reasons we say they are, and the things that bring us joy and fulfilment in life work exactly the way we’ve always said they do. That, in and of itself, is really good news.
Because this study is something we can point to with authority when we need backup.
And these days? Backup is good.
I've been looking over the results as they've been released. And with my bare two years of experience. (yes, it's been two years this month now!), what is being reported dovetails with experience nicely.
I think your theory on surgery bottlenecks has some merit to it. Yes, there is (for now) more access to surgical options and more and more insurance companies are paying for it (and some states mandate coverage still). But there is a wait time that can be daunting. I'll use my own experiences so far to illustrate:
From initial request for orchiectomy (August 2024) to consultation (January 2025) was five months. From consultation to proceedure (April 2025) was an additional three months.
There are 3-4 good surgeons in the region doing FFS. The top one doesn't make many forms of insurance. The second top rated one is who I have scheduled. From initial request (August 2024) to consultation (January 2025) was five months. Second consultation was March 2025, so two more months. Insurance approval for *most* of it was in May 2025, and the parts that have been denied are being appealed. Date of surgery is scheduled for November 2025. So 15 months for he best surgeon in the region that takes my insurance.
As for GRS? I decided that yes, I want to go that route in December 2024. Did my homework, and decided on the type I want (PPV). Insurance will only approve in the region, and there is *ONE* place doing that in a 400 mile range. Got the referral in March 2025, did the paperwork, and I have a consultation for my initial appointment.....for October 2026. 19 months later, and up to 3 years wait time. Even if I "settled" for my second or third choice options, I'm still looking at 2-4 years wait time.
Add to that there is now a push to get as much done NOW while you still can and yeah....bottlenecks and wait times are insane.
Thanks for posting.
In Australia we definitely have huge bottle-necks particularly around bottom surgery (both MTF and FTM) with only 7 or so surgeons available between MTF and FTM. Unlike USA we have to pay nearly the entire amount out of pocket as private insurance does not cover it and Medicare does not either.
There has been reports of GCS/SRS surgeries will be covered in the future (mid next year) under Medicare, but with so few surgeons the already 2 year waiting is will blow out even further.