


What do WPATH Standards of Care 8 actually say?
From The Blue Bird App

Foreword
This megathread was massive. I’m doing minimal work to curate here, and I’m not going to reproduce all of the screenshots the original megathread had. To find any of these items, check out the actual Standards of Care document, and go to the appropriate chapters. I have also pruned my coverage of one or two chapters, because I misunderstood a couple of things, and people better educated then I have corrected me.
The thread this all originated from was produced in a flurry, immediately after SoC8 came out. They include personal commentary. They are not complete, because I am not an expert on everything covered in it—for instance, intersex issues.
That said, this does cover the fundamental requirements that your doctors and insurers should be obliged to follow.
GLOBAL APPLICABILITY
“Global" here is best understood as "universal/foundational."
The chapter opens with an extensive discussion of the western-centric reality of worldwide discussions about gender, and how that has made a lot of gender work elsewhere much more difficult. Glad they acknowledge this.
I'm splitting the concrete recs out from the next bit, because the next bit makes me really happy, and y'all won't need me translating for it. These recs are simple. Localize in a culturally thoughtful manner, provide healthcare, know that laws often complicate things.

Here's the happy bit. Four sets of principles which should apply in ALL gender care.
Set 1:
Respect diversity, bodily autonomy, and provide the highest possible standard of care. Never pathologize trans identities.
Be. Empowering. And. Inclusive.

Set 2:
Involve trans people in the DESIGN of our own heathcare.
Affirm peoples' genders and reduce dysphoria "IF THIS IS PRESENT." That means that WPATH rejects dysphoria as the definitive part of a trans identity.
Reject all conversion-type therapies, no matter what.
Set 3:
Providers need to educate their own damn selves! - Customize treatment to each individual patient's needs!
Promote well-being. Dysphoria may not even be present!
FULL AND INFORMED PARTICIPATION OF TRANS PATIENTS IN HEATHCARE!!
Reduce administrative interference.

Maybe it's just me, but seeing WPATH stand up and shout from the rooftops that the paternalistic approaches we're all used to need to be discarded makes me really happy. For the first time, I feel seen by WPATH, not gatekept.
SUMMARY OF HRT/SURGICAL REQUIREMENTS
1. All criteria presented here should be personalized as appropriate. They're a base to work from, not a prescription.
2. Dysphoria is NOT REQUIRED FOR ANYTHING. WPATH required Gender Incongruence, per WHO and ICD-11
HRT Requirements:
1. You're gender incongruent.
2. You can consent.
3. There's no other apparent cause (before you get mad, Trans OCD is a thing; this needs to be here)
4. You understand what HRT will do to you. Summary: WPATH endorses informed consent as standard.
Surgery (ALL SURGERIES!!) requirements:
1. All HRT requirement items.
2. Where relevant, you understand how surgery could affect fertility.
3. You've been on HRT for 6 months, except where HRT isn't safe (E and T allergies are rare, but exist) or is NOT DESIRED!
NO LETTER!
Wherever letters are needed by outsiders: Any medical professional with a Master's or higher and experience in gender care can write a letter. ONLY ONE. EVER.
For kids (Blockers/HRT):
1. Adult HRT requirement items
2. Parents must be involved.
3. Must demonstrate cognitive maturity
4. Must have hit Tanner 2 (early puberty).
5. Fertility counseling.
No age ranges-each patient should be assessed individually based on their biology.
For kids (Surgical):
1. All kids' HRT requirement items.
2. 12 months HRT before any surgery (unless it's not safe or desired).
No age restrictions in the overview (parental approval is still required).
SURGERY CHAPTER
Some very strong statements on the medical necessity of transmasc AND transfem top surgery. Extensively cited.
FFS has been rebranded Facial Gender Affirming Surgery (FGAS) to be inclusive of Facial Masculinization Surgery and is as extensively cited. These statements are very strong. It makes sense, since Dr. Capitán, of FacialTeam, chaired this committee, but this statement reads like one major objective for this chapter was to force coverage for FGAS. It also rolls facial hair removal into FGAS.
Trach shaves, vocal chord surgery, all top surgery types, BODY CONTOURING (!!!), hair removal, all bottom surgeries including penis-preserving vaginoplasty and prospective penile transplants for transmascs--this list is MASSIVE.
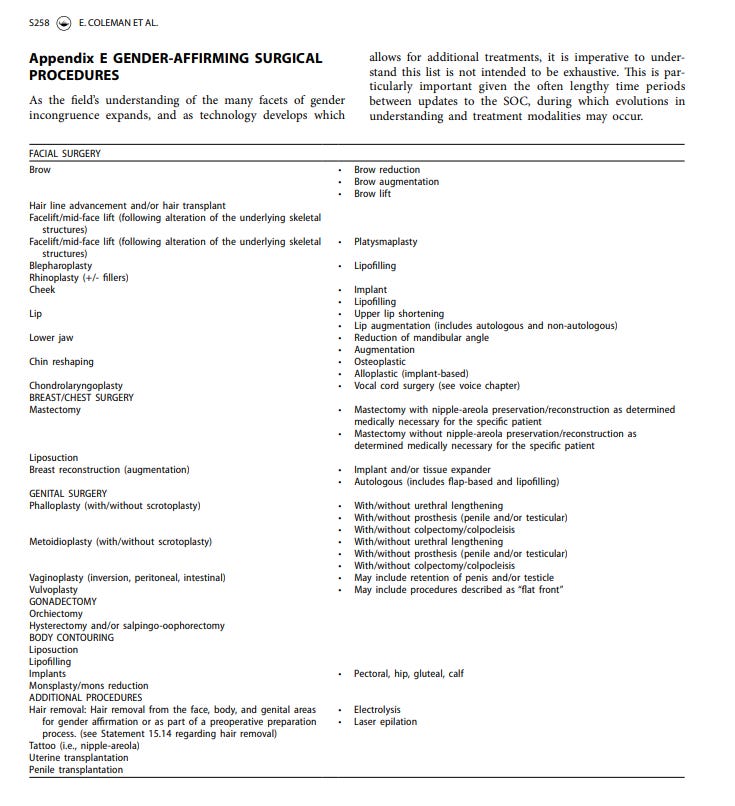
6 months on HRT (unless it's not safe or not wanted) before ANY gender affirming surgery. The SoC strongly recommends some sort of hormone after any procedure which removes gonads. Given stroke and osteoporosis risks without either/both good E or T levels, this is smart.
SoC8 also recommends FOR surgery for kids--but also expects a multidisciplinary care team (i.e., they're going to want therapists in on this and cross-checking each other's work). Tedious, but sensible.
Strong recommendation for individualized surgical plans--strongly inclusive of procedures like nullification, vagina-preserving phalloplasty, etc. Demands that surgeons work WITH patients--they want us at the front of our own decisions.
HRT CHAPTER
This chapter is meant to apply to both adults and kids, but kids on HRT are also subject to the adolescent chapter. Very important note. But pubertal HRT is very firmly endorsed.
SoC8 says there's no real evidence to support progesterone as part of HRT, but later notes that if a patient is aware of risks, that it's OK. This is correct--there's only ONE study (low dose and only 3 months long!) on the effects of progesterone right now. The data's not there. Also recommends against oral estrogen for anyone at blood clot risk or older than 45--injectable, patch, or gel instead. That's good medicine, but ye gods, that's gonna put a hell of a pinch on the injectable estrogen supply in the United States.
No mention of letters or assessment anywhere (and IIRC the Assessment chapter recommends against letters for HRT). Recommends AGAINST stopping HRT before gender-affirming surgery.
Throw a party, thank god! These are loooong overdue.
NONBINARY CHAPTER
They define enby identities very broadly here, but note that the term is used mostly in the West. They openly acknowledge colonial, racist genocide of indigenous genders on the FIRST PAGE of the chapter.
Side note: I really like non-linear spectrum as a description for gender diversity. The community has really struggled, in my opinion, with terminology to describe the weird, amorphous cloud that gender is, and NLS brings to mind something more like this picture, to me.

WPATH dunks on providers relying on patients--esp. enbies--for educating them. It also demands individualized care based on the individual gender of the person. It also demands doctors and clinics be well-educated on gender diversity, not just binary modes.
I almost want this to just stand on its own without comment, because it's so beautiful.
But, in a nutshell, unless HRT is a physiological necessity for a specific surgery (like metoidioplasty), WPATH says HRT isn't required for enbies before surgery.

ASSESSMENT CHAPTER
Assessment opens with some basic stuff, then this on Informed Consent, which probably seems really wishy-washy compared to what one might hope. I don't read it that way. Some nations have gatekeeping by law, & WPATH needs to serve those nations too.

Note that second paragraph specifically. This is an endorsement of informed consent where possible by law, and emphatically encourages trans people be part of the conversation. This is as far as they can really go and still have these SoC's function in those countries.
WPATH specifically recommends against therapy before HRT or surgery. They recommend therapy when we ask for it, but against it in all other circumstances. They also advocate for ready, easy, quality access to HRT & surgery. They're tearing down the gates here, people. Wow.
Many of the basic recommendations in the Assessment chapter are not a large move from SoC7 aside from pulling back on gatekeeping where permitted by law. There are some... interesting... items in their recs, though--specifically 5.4, 5.5, & 5.7.
5.4: This section is much less problematic than the header recommendation looks, and here's why: SoC documents must rely on data to make recommendations, and trans people who don't socially transition are almost unstudied. Ethically, they HAVE to recommend what they have evidence for.
5.5: The header looks like they're requiring one letter for everything, but the substance of the recommendation doesn't bear it out--it's one letter where required. It also throws credentialing out the window, so no more "gotta have a PsyD" nonsense.
5.7: This is also better than it looks, but still damn weird. They're rolling evolving gender identities and genderfluidity into detransition. That said, it overtly rejects detransition being a regret-filled thing, which is very good. The reason they’re doing this is this: the proportion of the population who are trans is rising, which means an explosion in total headcount. If detrans rate is 0.2%, say, that means the detrans total headcount will also explode even if the proportion doesn't change. They're heading off the weaponization of detransitioners at the pass here--saying there's lots of reasons, it's not tragic, and that there needs to be robust support for people who do detransition. And frankly, it's a good stance. I agree.
ADOLESCENTS CHAPTER
A personal note: I think this chapter was probably one of the reasons for the extreme delays in SoC8 being published.
Let's start with pissing off TERFS, which is one of my favorite things to do. This is a very polite, scholarly way of saying that the TERF stance of "there's no such thing as a trans child" is stupid beyond belief.
Which it is.

TERFs and reactionary-rights are going to riot on this one: all age recommendations have been stripped out. That means there's no longer an age prohibition in the WPATH SoC's on surgery. All surgery. This is important because age of majority differs from country to country & WPATH has to serve the whole world. I expect the right is going to absolutely melt down over this, because even parental consent has the asterisk "unless [parental] involvement is determined to be harmful to the adolescent," which transphobic far-right parents will be.
ROGD & Littman are still mentioned in SoC8, but the SoC's specifically dispute them. It's a much more wishy-washy statement than I'd prefer, and leaves the door open to people suggesting someone convinced their kid they're trans. They resist stuff like ROGD, but not strongly.
Surgery for adolescents is assumed as being a thing that happens regularly under 6.11. and 6.12. And bottom surgery is listed as a procedure teens are eligible for.

In general, a lot of the recommendations mirror corresponding adult chapters (covered elsewhere), or tweak those guidelines to involve parental oversight, longer waits, and practitioner cross-checking. It's irritating and slow, but I get it. I'm not a fan, but I get it.
A lot of what this chapter seems to be doing is threading the needle to open up gender-affirming care for teens while placating transphobic parents and lawmakers where they can. There's a nice and extended call to arms to normalize trans identities in schools and communities, though. Big fan of that. There's also a terminologically-generic ban on conversion therapy. So much for "Gender Exploratory Therapy." Lots of basic "educate people" recs too.
6.11: This section is all about getting parents on board with their kids' gender identity. It even calls out mismatches in reporting on a teen's gender between the teen themselves and their caregiver as being a big flag. And it rejects ROGD as an artifact of bad parenting. But the big money comes at the end. Make no mistake: what they're saying here is that big, sustained transphobia is child abuse, and if transphobic parents dig in, to get Child Protective Services involved.
In other words, removing the child from their custody.
6.12b: Item B advocates for a slow, careful approach to teen transition, but also encourages blockers to buy that time. It affirms parental/patient reporting of gender histories where it's not in earlier medical records.
6.12c: Item C is essential. Long-term, abstract thought is a structural development of the adolescent brain, and it's unethical to endorse HRT/surgery until the teen has developed the ability to make those assessments. People might buck against this, but I think it's dead on. What's better is that the SoC establishes concrete mileposts to judge this readiness by, and specifically divorces the ability from age. Some kids are going to have this capacity at 14. Some won't have it at 17. Biology is messy.
6.12g: Surgery. Inclusive of bottom surgery. Yep, it's in there. WPATH generally advocates for later timeframes for surgeries ("After 18 with exceptions in some cases"), but they've left those rails off specifically so that, as research matures, younger kids can access surgery.
WPATH then talks about risks of long-term use of blockers, *and then suggests HRT as an appropriate solution*. Wow, that argument blew up in TERFs' faces. AND THEN WPATH cites transphobic violence as a reason FOR teens getting surgery if they need it.
In summary: there's some REALLY questionable stuff that gets cited in the precede of this chapter that, it seems to me, is a remnant of the draft version's total insanity, but little is incorporated into the actual rec's.
There are training wheels, but this is liberation.
CHILDREN CHAPTER
For clarity: this is for prepubescent kids. WPATH opens by saying "childhood gender diversity is an expected aspect of general human development [&] childhood gender diversity is not a pathology or mental health disorder."
Let's GO!
There is a flat repudiation of conversion therapy and similar as coercive. Gender-affirming care for kids "promote[s] a trajectory of well-being that will sustain them... during the transition to adolescence."
The recommendations in this chapter are very simple: educate, provide support for kids and their families, and *maybe* do social transition. Super low-risk stuff, all age- and developmentally-appropriate. Still, there's interesting stuff here.
7.3: This is one of the most interesting autism/trans overlap statements I've read yet, and it comes from a position of 'these kids are very young, and autistic trans kids can struggle to articulate their feelings.' As a result, therapists who work with trans kids need specific, extensive training in autism in young kids. 100% agree and support. Given the incidence rate, I kind of wish this were in with teen and adult recommendations too.
7.5: This is the best repudiation of ROGD yet, and it doesn't even mention Littman. 'No using single sources, and you're not allowed to discourage kids' genders.' Generally, these assessments seem designed to help prep the ground if the kid turns out to be trans. Very sensible.
7.8: WPATH recommends therapy for PARENTS AND FAMILY MEMBERS of trans and potentially-trans children! Yes, this is just plain sensible, but dear god, the difference a really well-supported and -informed parent can make!
7.9: Why stop there? Let's connect with the kids' teachers, coaches, and religious leaders too, and make them part of the active support network! This is a level of support that'll let trans kids grow up loving their transness. Holy crap, I'm in love.
7.11: Trans kids deserve sex ed which fits their bodies *prior to puberty*. I mean, yeah, duh, but this is a wonderful idea and I think I can hear Ron DeSantis having an aneurism already.
7.12: This section says that if a kid is ready, they can start a social transition, they can and should. There's no sound data supporting delay. They do recommend a "consistent articulation of a gender identity," which IDK how I feel about, given autism questions.
7.14 This section is huge, and I know why. They're overtly rejecting the TERF "I touched the wrong toy and they transed me" strawman, and they're doing it quite robustly. There's a lot here about the uncertainty of gender in a developmental sense, and that's really good because gender as a fixed, long-term, abstract concept is connected to brain development. Different young kids develop at different rates, but some will explore this stuff and turn out cis. That's expected, given brain development patterns. This section appears to be an extended "how do I navigate that developmental challenge while also being gender affirming for my possibly-trans kid?" guide.
And that makes sense. It's tricky and uncertain, and you want the kid to grow up happy and healthy no matter who they become.
No joke, the Children chapter is my favorite so far. In fairness, there's really no controversies to navigate, but these are support structures that'll make for kids who *know* they're loved and supported by their family. That's always a good thing.
MY PERSONAL BOTTOM LINE ON SoC8
SoC8 isn't perfect. But—and this is my personal judgment without having had time to check references—it is a quantum leap forward for us. I think they tore down the gates as much as they could and still be accepted around the world.
These Standards of Care taste of freedom to me.
They repudiate the right. They repudiate TERFs. They repudiate transmedicalists.
For the first time, I feel like WPATH is on my side, rather than standing against me. And it feels good to have a strong ally. It feels really good.